Steroid injection therapy for knee osteoarthritis
How steroid injection works
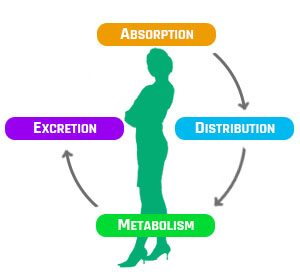
In 1951, Hollander et al. (1951) first described the use of intraarticular injections of corticosteroids for the management of arthritis, the Glucocortoids marked immunosuppressive and anti-inflammatory properties started a rapid global change in the treatment for joint conditions. The modified cortisol structure 16-alpha-hydroxyl-9-alphafluoroprednisolone was given the name triamcinolone, it is lipophilic and ubiquitous to humans so once delivered as a bolus it enters the target cells by passive diffusion (Scherer et al., 2014). The drug binds to specific receptors in the cytoplasm and DNA-binding domain, this up regulates and down regulates genes, changing transcription of proinflammatory mediators, effectively halting the prostaglandin inflammatory pathway and supressing its immune response (Rang and Dale’s, 2007). Some triamcinolone acetonide (steroid) may be absorbed into the systemic circulation from synovial spaces over a period of 2 to 3 weeks (Derendorf et al., 1986), clinically significant systemic levels after intra-articular injection are unlikely to occur, and it has a terminal systemic half-life of between 3.2 and 6.4 days (Scherer et al., 2014). Triamcinolone acetonide is a substrate of CYP3A4 and is metabolised largely hepatically (by the liver) so co-administration with strong CYP3A4 inhibitors eg, clarithromycin, is not recommended because it increases plasma corticosteroid levels and adverse effects may occur (EMC, 2018). The drug is eliminated by the kidney and is excreted in urine.
How effective are steroids compared to other injections?
Many RCT’s have been performed on intra-articular modalities for KOA, and in a very recent meta-analysis a comparison of efficacy and safety of intraarticular Hyaluronic acid and intraarticular corticosteroids was made (He et al., 2017). Two reviewers perform a robust electronic literature search and independently assessed fourteen studies using the modified Jadad scale, these RCT’s included a total of 1794 participants. As is typical in these reviews the heterogenous data meant a random-effects model of analysis. The results showed that at one month follow up intraarticular corticosteroids significantly reduced VAS pain score more than intraarticular Hyaluronic acid (p 0.03), but interestingly by three months follow up there was no difference between the drugs, then at six months the Hyaluronic acid was favoured. For the functional WOMAC outcome at 6 months again the Hyaluronic acid was best, but in the active knee flexion test for joint range of movement both were very beneficial but there was no significant difference between modalities. What is of clinical importance was in some trials intraarticular Hyaluronic acid caused more than double the topical adverse effects compared with intraarticular corticosteroids, but both methods were deemed relatively safe for practice (Leighton et al., 2014). Another systematic review of randomised controlled trials to evaluate the efficacy and safety of corticosteroids found twenty-eight trials, including 1973 participants (Bellamy et al., 2006). This review differed by finding a lack of evidence for efficacy in functional improvements in KOA but confirmed the short-term benefit (2-3 weeks) of IA corticosteroids are now well established, yet longer term benefits have not been confirmed. It also recognised that few side effects have been reported offering the treatments of KOA with intra-articular triamcinolone as safe.
I’ve read studies that have negative opinions of steroid injections
McAlindon et al., (2017) performed a two-year, randomized, placebo-controlled, double-blind trial of intra-articular triamcinolone vs saline, the aim was to compare the effectiveness of 40 mg/mL 1mL of triamcinolone against 1 mL of 0.9% sodium chloride for KOA. These drugs were delivered every three months to 140 patients, during which time participants underwent MRI scans, x-rays and x-ray absorptiometry, to assess bone density, cartilage and effusion changes. A mixed-model analyses revealed, knee pain reduction was no different between groups. Authors concluded a greater progression of knee cartilage volume loss in the triamcinolone group and no sustained effect on intra-articular inflammation as indicated by persistence of effusion. Clinically this provides very little support for the modality, and offers opposing opinions to that of the previous systematic reviews (Bellamy et al., 2006; He et al., 2017). There are some key constraints to the study methodology. The average age of the triamcinolone group participants was older, which could conceivable offer reason for a less successful outcome as chondrocytes with late-stage OA are vulnerable to apoptosis (Goldring and Goldring, 2007). Groups were asked to stop adjuvant pharmacological therapy such as anti-inflammatories but paracetamol was acceptable, the absence of a drug diary analysis to compare volumes taken between groups may have led to confounding variables. Another is the feasibility that saline can act as a treatment not just a placebo i.e. washout, so it is relevant that this group had more adverse effects, and the only case that was graded as severe. The drug triamcinolone was delivered at 40mg/ml alone, yet in practice it is often co-prescribed with lidocaine, also many injection therapists debate that dose is too little for a large knee joint, some prefer 80mg/ml, so the trial did not truly reflect a real-world consultation and has limited clinical application. Crucially this trial measures imaging and pain score outcomes three months after injections, yet it is well established that triamcinolone has an effect lasting less than this period, so they will have been missed. In summary this trial which refutes support for triamcinolone, compared modalities with questionable clinical relevance, measured bias from confounding pharmacological variables, was insensitive to treatment effects, and based conclusion on a comparison between two interventions delivered in the absence of a true control.
What’s the usual process for injections?
The treatment requires informed consent, to best achieve this the clinician should give a patient time to reflect on some patient information (ARC, 2018b; DOH, 2009). Choosing the patient is medically eligible for this procedure is essential, patient injection check list are commonplace and vary greatly, used prior to treatment it raises cautions, contraindications, side effects and key drug interactions (see appendix; (Local Formulary, 2018)). The treatment should be in stages and again there is some variation within the literature; firstly the environment and drug preparation, needle technique selection and mixing of the drug, safety aspiration and assessment, sharps disposal, wound after care and advice (WHO, 2010). The general consensus is that intra-articular injections adopt a strict aseptic, no touch technique, (Saunders and Longworth, 2006) and monitor the patient after delivery for 30 minutes to assess for drug reaction (Atkins et al., 2010). Triamcinolone acetonide (Kenalog) is safe to delivered by intra-articular injection in 5–40 mg per ml, with a recommended maximum dose of 80 mg in 2ml (BNF, 2016). It is often mixed with 3ml of 1% lidocaine hydrochloride rapid onset local anaesthetic as per local guidance (Local Formulary, 2018).
References
Adatia, A., Rainsford, K.D., Kean, W.F., 2012. Osteoarthritis of the knee and hip. Part I: aetiology and pathogenesis as a basis for pharmacotherapy. J. Pharm. Pharmacol. 64, 617–625. https://doi.org/10.1111/j.2042-7158.2012.01458.x
Allen, K.D., Golightly, Y.M., 2015. Epidemiology of osteoarthritis: state of the evidence. Curr Opin Rheumatol 27, 276–283. https://doi.org/10.1097/BOR.0000000000000161
ARC, 2018a. Musculoskeletal Calculator. Arthritis Research UK. NHS Dorset CCG. [WWW Document]. URL https://www.arthritisresearchuk.org/arthritis-information/data-and-statistics/musculoskeletal-calculator.aspx (accessed 4.30.18).
ARC, 2018b. Steroid injections patient information leaflet. Arthritis Research UK [WWW Document]. URL https://www.arthritisresearchuk.org/arthritis-information/drugs/steroid-injections.aspx (accessed 5.3.18).
Atkins, E., Kerr, J., Goodlad, E., 2010. A Practical Approach to Orthopaedic Medicine: Assessment, Diagnosis, Treatment, 3e, 3 edition. ed. Churchill Livingstone, Edinburgh ; New York.
Atkinson, K., Coutts, F., Hassenkamp, A., 2005. Physiotherapy in Orthopaedics, 2nd ed. Churchill Livingstone, Elsevier, London.
Bannuru, R.R., Natov, N.S., Obadan, I.E., Price, L.L., Schmid, C.H., McAlindon, T.E., 2009. Therapeutic trajectory of hyaluronic acid versus corticosteroids in the treatment of knee osteoarthritis: a systematic review and meta-analysis. Arthritis Rheum. 61, 1704–1711. https://doi.org/10.1002/art.24925
Bellamy, N., Campbell, J., Robinson, V., Gee, T., Bourne, R., Wells, G., 2006. Intraarticular corticosteroid for treatment of osteoarthritis of the knee. Cochrane Database Syst Rev CD005328. https://doi.org/10.1002/14651858.CD005328.pub2
BNF, 2016. British National Formulary. BMJ Group, British Medical Association & Royal Pharmaceutical Society, London.
Buckwalter, J.A., Martin, J.A., 2006. Osteoarthritis. Adv. Drug Deliv. Rev. 58, 150–167. https://doi.org/10.1016/j.addr.2006.01.006
Butler, D., 1991. Mobilisation of the Nervous System, 1e, First Edition edition. ed. Churchill Livingstone, Edinburgh.
Craft, J.A., Kurzweil, P.R., 2015. Physical examination and imaging of medial collateral ligament and posteromedial corner of the knee. Sports Med Arthrosc Rev 23, e1-6. https://doi.org/10.1097/JSA.0000000000000066
CSP, 2016. Expectations for injection therapy educational programmes. Chartered Society of Physiotherapy. [WWW Document]. The Chartered Society of Physiotherapy. URL http://www.csp.org.uk/publications/expectations-injection-therapy-educational-programmes (accessed 4.30.18).
CSP, RDSPT, 2018. Osteoarthritis of the Hip or Knee Guideline. Royal Dutch Society of Physical Therapy [WWW Document]. The Chartered Society of Physiotherapy. URL http://www.csp.org.uk/documents/osteoarthritis-hip-or-knee-guideline (accessed 5.4.18).
Derendorf, H., Möllmann, H., Grüner, A., Haack, D., Gyselby, G., 1986. Pharmacokinetics and pharmacodynamics of glucocorticoid suspensions after intra-articular administration. Clin. Pharmacol. Ther. 39, 313–317.
Dieppe, P.A., Lohmander, L.S., 2005. Pathogenesis and management of pain in osteoarthritis. Lancet 365, 965–973. https://doi.org/10.1016/S0140-6736(05)71086-2
DOH, 2009. Reference guide to consent for examination or treatment. 2nd Edition. Department of Health.
EMC, 2018. Kenalog Intra-articular / Intramuscular Injection – Summary of Product Characteristics [WWW Document]. URL https://www.medicines.org.uk/emc/product/6748/smpc (accessed 4.29.18).
Fink, B., Egl, M., Singer, J., Fuerst, M., Bubenheim, M., Neuen-Jacob, E., 2007. Morphologic changes in the vastus medialis muscle in patients with osteoarthritis of the knee. Arthritis Rheum. 56, 3626–3633. https://doi.org/10.1002/art.22960
Goldring, M.B., Goldring, S.R., 2007. Osteoarthritis. J. Cell. Physiol. 213, 626–634. https://doi.org/10.1002/jcp.21258
He, W., Kuang, M., Zhao, J., Sun, L., Lu, B., Wang, Y., Ma, J., Ma, X., 2017. Efficacy and safety of intraarticular hyaluronic acid and corticosteroid for knee osteoarthritis: A meta-analysis. International Journal of Surgery 39, 95–103. https://doi.org/10.1016/j.ijsu.2017.01.087
Hegedus, E.J., Cook, C., Hasselblad, V., Goode, A., McCrory, D.C., 2007. Physical examination tests for assessing a torn meniscus in the knee: a systematic review with meta-analysis. J Orthop Sports Phys Ther 37, 541–550. https://doi.org/10.2519/jospt.2007.2560
Local Formulary, 2018. Dorset Formulary. Dorset NHS [WWW Document]. URL http://www.dorsetformulary.nhs.uk/chaptersSubDetails.asp?FormularySectionID=4&SubSectionRef=04.07.03&SubSectionID=A100&drugmatch=2424#2424 (accessed 4.29.18).
McAlindon, T.E., Bannuru, R.R., Sullivan, M.C., Arden, N.K., Berenbaum, F., Bierma-Zeinstra, S.M., Hawker, G.A., Henrotin, Y., Hunter, D.J., Kawaguchi, H., Kwoh, K., Lohmander, S., Rannou, F., Roos, E.M., Underwood, M., 2014. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthr. Cartil. 22, 363–388. https://doi.org/10.1016/j.joca.2014.01.003
NICE, 2014. Osteoarthritis: care and management. Guidance and guidelines CG177. National Institute for Health and Care Excellence. [WWW Document]. URL https://www.nice.org.uk/guidance/cg177/chapter/1-Recommendations#pharmacological-management (accessed 5.3.18).
Petty, Moore, 2001. Neuromusculoskeletal Examination and Assessment: A Handbook for Therapists, 2nd ed. Churchill Livingstone, Elsevier.
Petty, N., Ryder, D. (Eds.), 2017. Musculoskeletal Examination and Assessment – Volume 1: A Handbook for Therapists, 5e, 5 edition. ed. Elsevier, Edinburgh.
Porter, S.B., 2003. Tidy’s Physiotherapy. Physiotherapy Essentials. Butterworth-Heinemann, Elsevier.
Prasad, N., Murray, J.M., Kumar, D., Davies, S.G., 2006. Insufficiency fracture of the tibial plateau: an often missed diagnosis. Acta Orthop Belg 72, 587–591.
Rang, H., Dale’s, M., 2007. Rang & Dale’s Pharmacology, 6th ed. Churchill Livingstone, Elsevier.
Rossi, L., Lascio, S.D., Kouros, M., Pagani, O., 2015. A rare avascolar osteonecrosis of the knee related to biphosphonate treatment in a patient with metastatic breast cancer. Breast Dis 35, 203–206. https://doi.org/10.3233/BD-150410
RPS online, 2017. BMJ study on risk of heart attack and NSAIDS RPS responds with online statement [WWW Document]. URL https://www.rpharms.com/news/details//BMJ-study-on-risk-of-heart-attack-and-NSAIDS—RPS-responds (accessed 5.4.18).
Saunders, S., Longworth, S., 2006. Injection Techniques in Orthopaedics and Sports Medicine with CD-ROM: A Practical Manual for Doctors and Physiotherapists, 3rd Revised edition edition. ed. Churchill Livingstone, Edinburgh London New York Oxford Philadelphia St. Louis Syndney Toronto.
Scherer, J., Rainsford, K.D., Kean, C.A., Kean, W.F., 2014. Pharmacology of intra-articular triamcinolone. Inflammopharmacol 22, 201–217. https://doi.org/10.1007/s10787-014-0205-0
Sellam, J., Berenbaum, F., 2013. Is osteoarthritis a metabolic disease? Joint Bone Spine 80, 568–573. https://doi.org/10.1016/j.jbspin.2013.09.007
Turkiewicz, A., Gerhardsson de Verdier, M., Engström, G., Nilsson, P.M., Mellström, C., Lohmander, L.S., Englund, M., 2015. Prevalence of knee pain and knee OA in southern Sweden and the proportion that seeks medical care. Rheumatology (Oxford) 54, 827–835. https://doi.org/10.1093/rheumatology/keu409
Valdes, A.M., Loughlin, J., Timms, K.M., van Meurs, J.J.B., Southam, L., Wilson, S.G., Doherty, S., Lories, R.J., Luyten, F.P., Gutin, A., Abkevich, V., Ge, D., Hofman, A., Uitterlinden, A.G., Hart, D.J., Zhang, F., Zhai, G., Egli, R.J., Doherty, M., Lanchbury, J., Spector, T.D., 2008. Genome-wide association scan identifies a prostaglandin-endoperoxide synthase 2 variant involved in risk of knee osteoarthritis. Am. J. Hum. Genet. 82, 1231–1240. https://doi.org/10.1016/j.ajhg.2008.04.006
Wang, H., Cheng, Y., Shao, D., Chen, J., Sang, Y., Gui, T., Luo, S., Li, J., Chen, C., Ye, Y., Yang, Y., Li, Y., Zha, Z., 2016. Metabolic Syndrome Increases the Risk for Knee Osteoarthritis: A Meta-Analysis. Evid Based Complement Alternat Med 2016. https://doi.org/10.1155/2016/7242478
WHO, 2010. WHO best practices for injections and related procedures toolkit. World Health Organisation [WWW Document]. URL http://www.ncbi.nlm.nih.gov/books/NBK138491/ (accessed 5.3.18).